La migraine est l’affection neurologique la plus fréquente chez la femme. Il convient de la rechercher systématiquement à l’interrogatoire avant la prescription d’une contraception hormonale et lors de toute consultation de suivi. Il est important de distinguer les migraines des simples céphalées de tension et d’en préciser le type (simple ou avec aura). Il faut également déterminer le caractère cataménial ou non des migraines.
L’évaluation du risque de migraine associé à l’utilisation d’une contraception hormonale est fondamentale, pour deux raisons :
- le caractère invalidant des migraines implique de ne pas aggraver les symptômes par un apport hormonal exogène inadapté ;
- le risque d’accident vasculaire cérébral ischémique est augmenté chez les femmes migraineuses utilisant une contraception œstroprogestative (COP).
Classification et critères diagnostiques des migraines
La migraine est une variété particulière de céphalée survenant par accès intermittents (crises) séparés par des intervalles libres. Il existe une classification internationale des céphalées permettant de distinguer les différents types de migraine (troisième classification de l’International Headache Society [IHS]).1
Migraine sans aura
La migraine sans aura répond à trois critères.
1 - Les crises de céphalée durent de quatre à soixante-douze heures sans traitement.
2 - La céphalée comprend au moins deux des caractéristiques suivantes :
- unilatéralité ;
- pulsatilité ;
- intensité modérée à sévère ;
- aggravation par l’effort physique.
3 - La céphalée est associée à au moins un des symptômes suivants :
- nausées et/ou vomissements ;
- photophobie et phonophobie.
Pour parler de migraine sans aura, au moins cinq crises remplissant les critères 1 à 3 sont nécessaires.
Migraine avec aura
L’aura est un ensemble de symptômes neurologiques focaux et réversibles, d’installation progressive, d’une durée inférieure à soixante minutes, précédant toujours une céphalée migraineuse.
Les trois types d’aura les plus fréquents sont :
- l’aura visuelle avec scotome scintillant (migraine ophtalmique), qui est de loin la plus fréquente ;
- l’aura sensitive avec des paresthésies ;
- les troubles du langage.
Le diagnostic de migraine s’établit par l’interrogatoire, permettant une description précise de la crise, d’apprécier son évolutivité et d’appréhender l’histoire familiale. L’examen clinique est normal. Il n’est pas nécessaire de réaliser une imagerie cérébrale.
Migraines cataméniales
D’après la classification de l’IHS, il existe deux types de migraine cataméniale :
- la migraine cataméniale dite « pure », caractérisée par la survenue de crises de migraine sans aura entre les deux jours précédant les règles et les trois premiers jours du cycle, apparaissant au moins lors de deux cycles sur trois, sans crise en dehors de cette période ;
- la migraine « liée aux menstruations » caractérisée par la survenue de crises de migraine sans aura entre les deux jours précédant les règles et les trois premiers jours du cycle, apparaissant au moins lors de deux cycles sur trois, associée à des crises avec ou sans aura survenant à d’autres moments du cycle.
Épidémiologie des migraines chez la femme
La prévalence globale de la migraine dans la population générale adulte varie avec l’âge. Elle est estimée à 14,4 %, avec une large prédominance féminine (sex-ratio 3/1). Chez la jeune fille de moins de 12 ans, elle est de 3 à 10 %. Puis elle augmente à la puberté, 10 à 20 % des migraineuses connaissant leurs premières crises à cette période. La prévalence atteint un pic entre l’âge de 35 et 39 ans, évaluée à 30 % chez les femmes, puis diminue avec l’âge.2
Plus d’un quart des femmes migraineuses constatent une association entre les crises migraineuses et les règles.3 Pour 8 % des femmes, il s’agit de migraines cataméniales pures alors que près de 50 % voient leurs crises migraineuses, tout au long du cycle menstruel, s’aggraver en période de règles. Elles sont plus fréquentes chez les femmes dont la migraine a débuté au moment de la puberté. La prévalence maximale se situe vers l’âge de 40 ans.
Contraception et risque de migraine
Il existe une association significative entre les migraines et l’utilisation en cours ou passée d’une COP, quelle que soit la combinaison utilisée et indépendamment de la dose d’éthinylestradiol (EE).4 Aucune étude n’a spécifiquement étudié le risque lié à l’utilisation des voies d’administration vaginale ou transdermique des COP ou des pilules les plus récentes contenant de l’estradiol ou de l’estétrol. La très grande variabilité interindividuelle de ce symptôme explique l’impossibilité de prédire l’évolution des migraines lors de l’utilisation d’une contraception hormonale.
Lors de l’utilisation d’un contraceptif, les migraines apparaissent le plus souvent dès les premiers cycles. Le risque de survenue de céphalée lors de l’utilisation d’une COP serait accru en cas d’antécédents personnels ou familiaux de migraine et augmenterait avec l’âge.5
La balance œstroprogestative de l’association hormonale de la pilule semble fondamentale.
Les contraceptions microprogestatives ne sont pas associées au risque de migraine.4 Une méta-analyse de quatre études observationnelles montre une diminution modeste mais significative du nombre mensuel, de la durée et de l’intensité des crises migraineuses ainsi qu’une diminution de l’utilisation de triptans liée à la prise de désogestrel.6 Il n’existe aucune donnée publiée sur la contraception progestative seule contenant de la drospirénone.
La littérature est très pauvre concernant le risque d’apparition ou d’aggravation des migraines cataméniales en lien avec l’utilisation d’une contraception hormonale. Il est donc difficile de déterminer si la contraception en elle-même exerce une influence supplémentaire et indépendante sur ce type de migraine.
Une étude prospective incluant 184 femmes a évalué le risque de survenue et la persistance de migraine cataméniale en comparant les utilisatrices d’une COP aux non-utilisatrices, en analysant spécifiquement la période prémenstruelle (comprenant les deux jours précédant les règles) et la période menstruelle, en différenciant les trois premiers jours du cycle et les derniers jours des menstruations.7 Dans cette étude, le risque de migraine était deux fois plus élevé pendant les trois premiers jours du cycle, indépendamment de l’utilisation d’une COP. L’utilisation d’une COP n’était pas associée globalement à une augmentation significative de la survenue et de la persistance des migraines cataméniales. En revanche, chez les utilisatrices de COP, le risque de migraine était significativement plus important en prémenstruel.
Risque d’AVC chez les patientes migraineuses utilisant une contraception hormonale
Contraception hormonale et risque d’AVC ischémique
Les résultats d’une méta-analyse publiée en 20138 montrent un doublement du risque d’AVC ischémique chez les utilisatrices de COP (risque relatif [RR] : 1,8 ; intervalle de confiance à 95 % : 1,2 - 2,8). Dans cette méta-analyse, lorsque le type de progestatif est pris en compte, le risque d’AVC ischémique est plus élevé avec les COP de première génération (qui ne sont plus commercialisées), comparativement aux non-utilisatrices, qu’avec celles de deuxième ou de troisième génération. Ces résultats diffèrent de ceux de la méta-analyse Cochrane en réseau publiée en 2015, qui ne semble pas établir de lien avec le type de progestatif mais qui montre plutôt une association significative entre les doses élevées d’EE et la survenue d’un AVC ischémique.9 Très peu de données ont été publiées concernant la voie d’administration non orale des COP, ce qui ne permet pas de conclure.10
Il n’existe pas d’étude épidémiologique de grande puissance ayant évalué le risque des COP contenant de l’estradiol ni de l’estétrol.
L’analyse de l’ensemble des études épidémiologiques évaluant l’association entre contraception progestative seule et risque d’AVC ischémique ne montre aucune augmentation de ce risque lié à l’utilisation de ce type de contraception, quelle que soit la voie d’utilisation.11
Migraine, contraception et risque d’AVC ischémique
Les migraines augmentent le risque d’AVC ischémique surtout chez les femmes souffrant de migraines avec aura (RR : 2,16 [1,53 - 3,03]).12 Un consensus européen a réanalysé en 2018 l’ensemble des données de la littérature concernant le risque d’AVC ischémique chez les utilisatrices de COP et mis en évidence un risque plus important en cas de migraine avec aura (tableau).13 Ce risque est encore plus important (odds ratio de l’ordre de 34) si la patiente est fumeuse.14 Il existe donc une synergie des facteurs de risque impliquant leur évaluation minutieuse avant toute prescription d’une COP chez la patiente migraineuse.
Quelle contraception en cas de migraine ?
D’après la révision récente des recommandations de la Société française d’études des migraines et céphalées :15
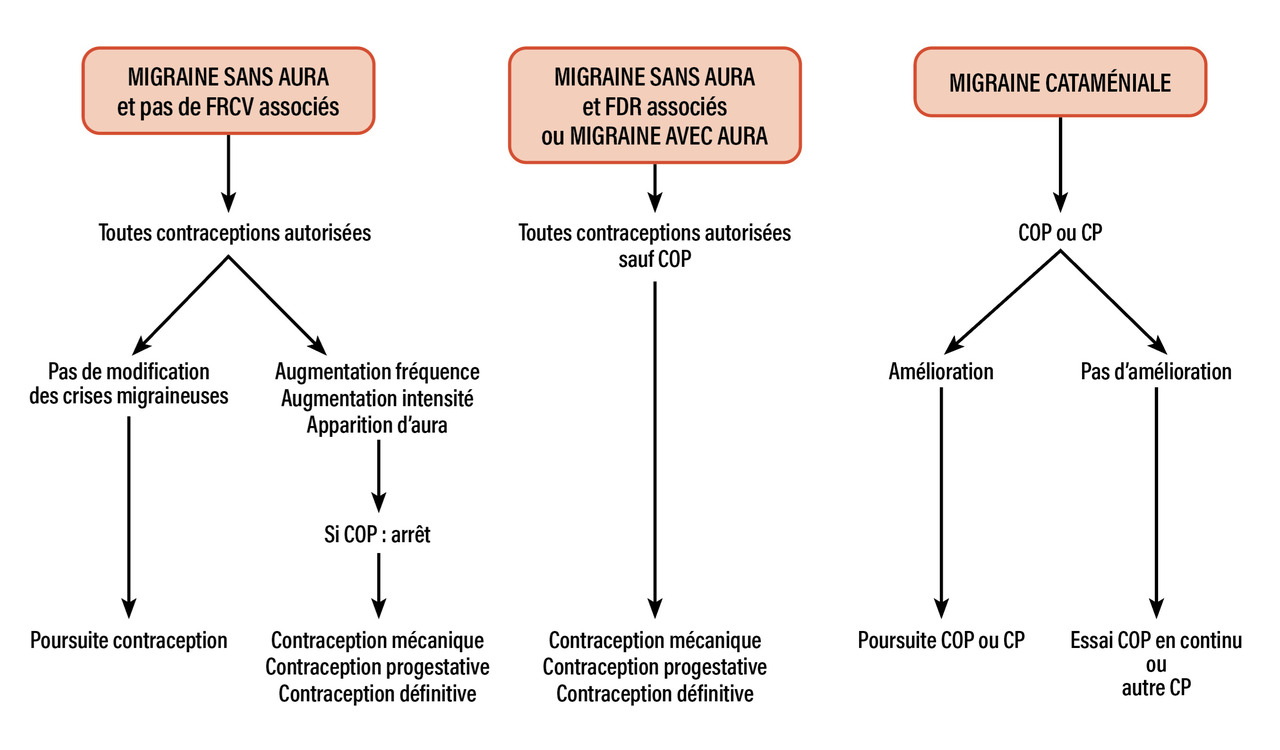
- la COP n’est, de principe, pas contre-indiquée en cas de migraine sans aura, en l’absence d’autres facteurs de risque artériel. Toutes les contraceptions sont potentiellement utilisables en l’absence de facteur de risque vasculaire ;
- la COP est contre-indiquée en cas de migraine avec aura ou en cas de facteur(s) de risque artériel associé(s) chez une femme ayant des migraines sans aura. La contraception fait alors appel aux autres stratégies contraceptives disponibles.
Les situations suivantes nécessitent d’arrêter la COP : céphalées persistantes de début récent, aggravation de la fréquence ou de la sévérité des céphalées, apparition de crises avec aura.
En cas de contre-indication à la COP, les alternatives sont l’utilisation d’une contraception orale microprogestative (désogestrel, drospirénone), d’un dispositif intra-utérin (DIU) au cuivre ou au lévonorgestrel ou une contraception définitive (à discuter en fonction de l’âge et du contexte clinique) [figure].
En cas de migraine cataméniale, l’utilisation d’une COP en continu, permettant d’obtenir une aménorrhée, diminuerait le risque. Par ailleurs, l’utilisation d’une COP plus faiblement dosée en EE ou à base d’estradiol ou d’estétrol, dont la fenêtre d’interruption est plus courte, pourrait constituer une alternative intéressante. Enfin, une autre solution serait l’utilisation d’une œstrogénothérapie percutanée pendant la fenêtre d’interruption de la COP.
Sous contraception microprogestative, on observe une diminution de l’apparition des migraines cataméniales pures, probablement en raison de l’aménorrhée souvent induite par ce type de thérapeutique contraceptive. La prescription d’une contraception progestative à pouvoir plus antigonadotrope contenant de la drospirénone, même si elle n’est pas évaluée, peut également être une option, en proposant un schéma continu sans prise des quatre comprimés placebos.
2. GBD 2016 Headache Collaborators. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2018;17:954-76.
3. Vetvik KG, MacGregor EA. Menstrual migraine: A distinct disorder needing greater recognition. Lancet Neurol 2021;20(4):304-15.
4. Aegidius K, Zwart JA, Hagen K, et al. Oral contraceptives and increased headache prevalence: The Head-HUNT Study. Neurology 2006;66:349-53.
5. Loder EW, Buse DC, Golub JR. Headache as a side effect of combination estrogen-progestin oral contraceptives: A systematic review. Am J Obstet Gynecol 2005;193:636-49.
6. Warhurst S, Rofe CJ, Brew BJ, et al. Effectiveness of the progestin-only pill for migraine treatment in women: A systematic review and meta-analysis. Cephalalgia 2018;38(4):754-64.
7. Lieba-Samal D, Wöber C, Frantal S, et al. Headache, menstruation and combined oral contraceptives: A diary study in 184 women with migraine. Eur J Pain 2011;15:852-7.
8. Plu-Bureau G, Hugon-Rodin J, Maitrot-Mantelet L, et al. Hormonal contraceptives and arterial disease: An epidemiological update. Best Pract Res Clin Endocrinol Metab 2013;27:35-45.
9. Roach RE, Helmerhorst FM, Lijfering MW, et al. Combined oral contraceptives: The risk of myocardial infarction and ischemic stroke. Cochrane Database Syst Rev 2015;2015(8):CD011054.
10. Lidegaard O, Lokkegaard E, Jensen A, et al. Thrombotic stroke and myocardial infarction with hormonal contraception. N Engl J Med 2012;366(24):2257-66.
11. Chakhtoura Z, Canonico M, Gompel A, et al. Progestogen-only contraceptives and the risk of stroke. Stroke 2009;40:1059-62.
12. Schurks M, Rist PM, Bigal ME, et al. Migraine and cardiovascular disease: Systematic review and meta-analysis. BMJ 2009;339:b3914.
13. Sacco S, Merki-Feld GS, Aegidius KL, et al. Correction to: Hormonal contraceptives and risk of ischemic stroke in women with migraine: A consensus statement from the European Headache Federation (EHF) and the European Society of Contraception and Reproductive Health (ESCRH). The Journal of Headache and Pain 2018;19:81.
14. Chang CL, Donaghy M, Poulter N, and World Health Organization. Collaborative study of cardiovascular disease and steroid hormone contraception. BMJ 1999;318:13-8.
15. Ducros A, de Gaalon S, Roos C, et al. Revised guidelines of the French Headache Society for the diagnosis and management of migraine in adults. Part 2: Pharmacological treatment. Rev Neurol (Paris) 2021;177:734-52.